SOAP Notes for Speech Therapy: The Ultimate Guide

SOAP Notes. Whether you’re a new grad or seasoned clinician, perfecting your treatment note is a crucial part of any speech therapist’s practice.
Speech therapy SOAP notes document important data and paint a picture of how the client participated in a session. That’s not always easy. A speech-language pathologist’s (also known as “SLP”) schedule is often filled with back-to-back clients throughout the day.
Having a clear understanding of what SLP SOAP notes are, and how to write one both thoroughly and efficiently can be a huge help to SLPs. This helps them feel confident that they documented the necessary information for insurance and legal purposes while not falling behind on paperwork or getting backed up on time.
What is an SLP SOAP Note?
SLP SOAP notes are a written document that reports on what was done in a therapy session. It should be written the same day as the session occurred. This timely documentation ensures accurate and up-to-date documentation is completed. Additionally, SLP SOAP notes must be completed the same day as the service because they are attached to charges for the session.
The SOAP note can be written after the session. Or, if the SLP uses an easily accessible, concise SOAP note template, the note can be written during the last few minutes of the session itself. TheraPlatform offers a built-in SLP SOAP note template that is clear, consistent, and concise. This allows SLPs to complete the soap note template during the session, making documentation with back-to-back therapy sessions a breeze.
What’s in a SOAP note?
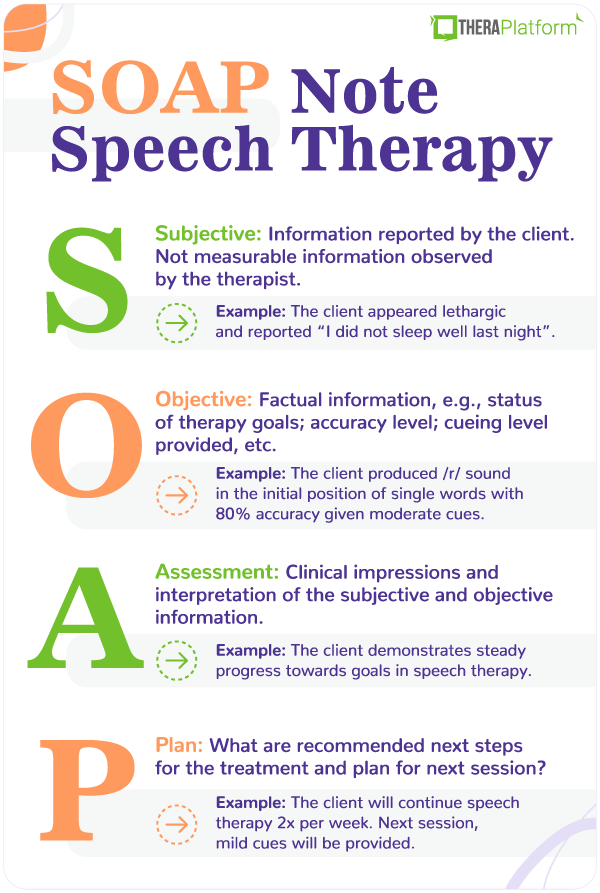
SOAP stands for the 4 sections that make up the therapy note: Subjective, Objective, Assessment and Plan.
It may be shared with the client and/or his or her caregiver, as well as insurance companies. Here’s a closer look at what makes up a SOAP note, and the do’s and don’ts to keep in mind when writing each section along with a SOAP note example.
Subjective
This is a brief statement that describes a client’s state from the therapist’s point of view.
The information in this section isn’t measurable, and can be gathered both from the therapist’s observations and any information given by the caregiver who accompanies the client to the session.
What questions can you answer in the subjective section of your speech therapy SOAP note?
- Behavior (e.g., frequent refusals, cooperative, engaged, attentive)
- Medical status (e.g., recent illness)
- Current state (e.g., alert, lethargic/tired)
Do’s of writing the subjective section
- Keep it brief (about 1-3 sentences)
- Back up statements with supporting information such as quotes. (e.g, Mother reported “he woke up early and is tired today.”)
- Paint a clear picture of how the client participated in the session
Don’ts of writing the subjective section
- Make it too lengthy
- Include information that is irrelevant or unnecessary
Speech therapy SOAP note examples: Subjective section
1. Johnny appeared alert, and transitioned into the therapy room without difficulty. He was engaged and participated in all therapeutic activities that were presented.
2. Alice became upset and clung to her mother upon entering the therapy room. She frequently put her head down and refused to participate in tasks.
3. Cayden appeared lethargic and his mother reported, “he didn’t sleep well last night”. He was engaged and interactive when provided with positive reinforcement and praise.
Start your free trial now
Objective
The objective section is all about stating the facts. The information an SLP writes here must be measurable or quantitative. This usually includes reporting on therapy goals and stating the data that the client achieved for each goal targeted during the session.
When thinking of this section, think percentages, numbers, accuracy level, and scores.
Here, the speech-language pathologist will also state whether each therapy goal was targeted, not targeted, met, not met, or progressing.
What questions can you answer in the objective section of your SOAP note?
- Short term/current therapy goals
- Data reporting the client’s performance on each goal (percentage accuracy or number of times the client performed the targeted task)
- Cueing level provided for each goal (for example, maximum, moderate, minimal cues, or independently)
- If the goal was met or not met for that session
- Number of consecutive sessions in which each goal achieved has been met (e.g., 1 out of 3 consecutive sessions)
Do’s of writing the objective section
- Be clear and concise
- Include measurable data
- Report on the client’s performance
- Address each current therapy goal (if not addressed, mark as “not targeted”)
Don’ts of writing the objective section
- Don’t include lengthy descriptions of the therapy activities.
- Don’t write subjective information that cannot be quantified
Speech therapy SOAP note example: Objective section
1. Johnny produced the /r/ sound in the initial position of single words with 80% accuracy given moderate cues. (Goal Met for 2 out of 3 consecutive sessions)
2. Olivia identified common objects in 7 out of 10 opportunities given minimal cues. (Goal Progressing/Not Met)
3. Allison used irregular past tense verbs at the sentence level with 50% accuracy independently. (Goal progressing/not met)
Assessment
In the Assessment section of a SOAP note, a speech-language pathologist analyzes and interprets the information documented within the first two sections (the Subjective and Objective sections).
What questions can you answer in the Assessment section of your SOAP note?
- Is the client making progress towards goals overall?
- Are there any barriers to progress? For example, medical status, attendance, or the client’s behavior?
Do’s of writing the assessment section
- Note client’s response to receiving speech therapy (e.g., positive)
- Compare client’s performance to that of previous sessions
Don’ts of writing the assessment section
- Restate information already reported on in the subjective or objective sections
SOAP note example: Assessment
1. Ethan continues to demonstrate steady progress towards goals in speech therapy.
2. Logan’s behavior is impeding his progress towards goals in speech therapy.
3. Mila’s production of the /th/ sound improved by 15% compared to her previous session.
Get your free SOAP notes template
Plan
In this final section of the SOAP note, the therapist writes the recommended next steps for the client’s treatment.
These questions should be answered in the plan section of your SOAP note:
- Is continued treatment recommended?
- Should the client be discharged from speech therapy services?
- Are there any recommended changes to the treatment plan? If so, why? (e.g., a reduction in therapy from 2 times per week to 1 time per week due to the client’s progress towards therapy goals).
- Are there any other therapy services recommended going forward for this client? For example, “It is recommended that the client receive a formal audiological evaluation to rule out hearing difficulties”.
When writing the plan section, do:
State any recommended changes for the next therapy session. For example, “The next therapy session will focus on recording Alex’s speech and encouraging him to monitor it for articulation errors”.
And the don’t:
- Forget to back up your recommendations.
SOAP note example(s): Plan
- Client is approaching goal status for /r/ articulation. In the next session, /r/ words in the medial section will be introduced.
- Continue with current plan and evaluate each week
How to write a SOAP note
One part of writing a SOAP note is knowing what information to include. The other part is knowing how to document this information. Remember, clear, consistent, and concise are words an SLP should keep in mind when writing a SOAP note.
The benefits of writing session notes (SLP SOAP notes) in this way include:
- The therapist can easily refer to SLP SOAP notes from the previous session to compare progress.
- Parents and caregivers are able to better understand speech therapy goals and how the client is performing in sessions.
- Other professionals working with the client (e.g., teachers, occupational therapists, and ABA therapists) can view his or her therapy plan for speech.
- Required documentation can be more easily located by insurance providers and reviewers for reimbursement purposes.
- Now, let’s look at what those characteristics mean, and how SLPs can apply them to their daily notes.
Clear SLP SOAP notes
What does this mean for your SLP SOAP note?
You want to write it in a way that readers can easily understand the information. Some clinical terminology will be used. However, the note should describe the client’s performance during a session in a way that others who may not have a clinical background can still understand.
Let’s take a look at a clear SLP SOAP note example vs. a SOAP note example that is less clear.
Clear
Objective: Client produced the /r/ sound in the initial position of single words with 80% accuracy given moderate cues. (Goal met for 2 out of 3 consecutive sessions)
Not Clear
Objective: Client was able to accurately produce /r/ while reading a story about rabbits. He had more difficulty producing the final /r/ than the medial /r/, and was stimulable for corrections with verbal and tactile cueing. Client was excited that he will have a baseball game today. He liked the book but started crying during the game.
In the second, less clear SOAP note example, the longer description of the client’s performance is unclear to the reader. The specific goal targeted is not easy to determine. The reader is unsure of what word position the goal is for the /r/ sound to be produced.
The objective section in the less clear SOAP note example also leaves the reader questioning at what level the sound is being targeted (ex: single words or sentences). The second SOAP note example also includes extraneous information that is not clinically relevant. Professionally worded statements about the client’s state (ex: engaged, uncooperative) should be included in the “Subjective” part of the SOAP note.
The first, clear SOAP note example on the other hand, would be easier for the audience to understand. Only the most important clinical information is included. The objective section here clearly states the target sound, word position, level of hierarchy, and percentage that provides an objective report on the client’s performance.
Keep the purpose in mind
Another reason speech pathologists should keep their SLP SOAP notes clear? To fulfill the purpose of the note. The purpose of SLP SOAP notes is to clearly and accurately document a client’s diagnosis, the treatment being provided, and his or her progress.
Consistent SLP SOAP notes
SLP SOAP notes should appear consistent over time. If a client is seen for ongoing therapy at a given frequency (ex: weekly or monthly), the format of the SLP SOAP notes should look standardized. The specific clinical information such as the therapy goals, client’s state, and progress, will of course differ from one session to the next.
Using a SOAP note template makes it easy for an SLP’s SOAP notes to appear consistent overall. For one thing, it is simple for the SLP to input information about the session into a SOAP note template. Secondly, when using a SOAP note template, others can track and compare documentation over time. This can be important for the reader (such as an insurance reviewer) to easily compare documentation over a span of time to see if the client is demonstrating overall progress by receiving speech therapy.
Consistency with SOAP note templates means information is documented in the same place and format from one session to the next.
Concise SLP SOAP notes
SLP SOAP notes should be concise.
Documenting only the clinically relevant, most pertinent information about a session provides the following benefits:
- It is easier for the reader to locate information.
- It appears professional.
- Concise SLP SOAP notes help ensure only the most important clinical information is included.
How long should SLP SOAP notes be?
SLP SOAP notes should contain approximately 1 small paragraph per section. Some sections may have more information than others.
- Subjective: This section will likely contain 1-2 sentences describing the client’s state. For example, “Hannah was alert and engaged. She participated in all activities presented.” Or, “Owen appeared tired and required cues to participate in the therapy session. Mother reported he has been sick this week.”
- Objective: This will likely be the longest section of an SLP’s SOAP note. Since this is where the goals will be listed and reported on, the length will depend on how many current goals are being targeted in therapy.
- Assessment: The assessment section will likely contain approximately 4 to 5 statements. If the SLP uses a SOAP note template, this could be completed by marking checkboxes of statements that apply to the client’s current status in therapy.
- Plan: This is a short statement or two that will likely be bulleted and includes plans for future sessions.
For example, the SLP may only need to check boxes of statements on a SOAP note template that provide statements such as, “Recommend continue therapy per plan of care”, or “Client continues to demonstrate improvements in Speech Therapy.”
The entire note itself should not exceed 1 to 2 pages. Remember, to serve its purpose to provide parents, other professionals, and insurance reviewers necessary clinical information, the note should be succinct.
SOAP note example: Entire note
Using an SLP SOAP note template makes writing notes fast, efficient, and comprehensive. Here’s a complete SLP SOAP note example:
S: Johnny appeared alert, and transitioned into the therapy room without difficulty. He was engaged and participated in all therapeutic activities that were presented.
O: Client produced the /r/ sound in the initial position of single words with 80% accuracy given moderate cues. (Goal Met for 2 out of 3 consecutive sessions.) Client used personal pronouns accurately in 6/10 opportunities given minimal cues (Progressing/Goal not met.)
A: Johnny continues to demonstrate steady progress towards goals in speech therapy.
P: It is recommended Johnny continue with the current treatment plan of 2 times per week for 30 minutes per session, for an estimated duration of 180 days.
How EMR software can help with speech therapy SOAP notes?
Electronic medical record (EMR) and practice management software, such as TheraPlatform, can help make note taking fast, flexible and accurate.
Benefits of using EMR for speech therapy notes
Consistent notes with a library of note templates
Having an EMR with built-in note templates, such as SOAP, can help speech-language pathologists stay organized and write more consistent and concise speech therapy notes each time.
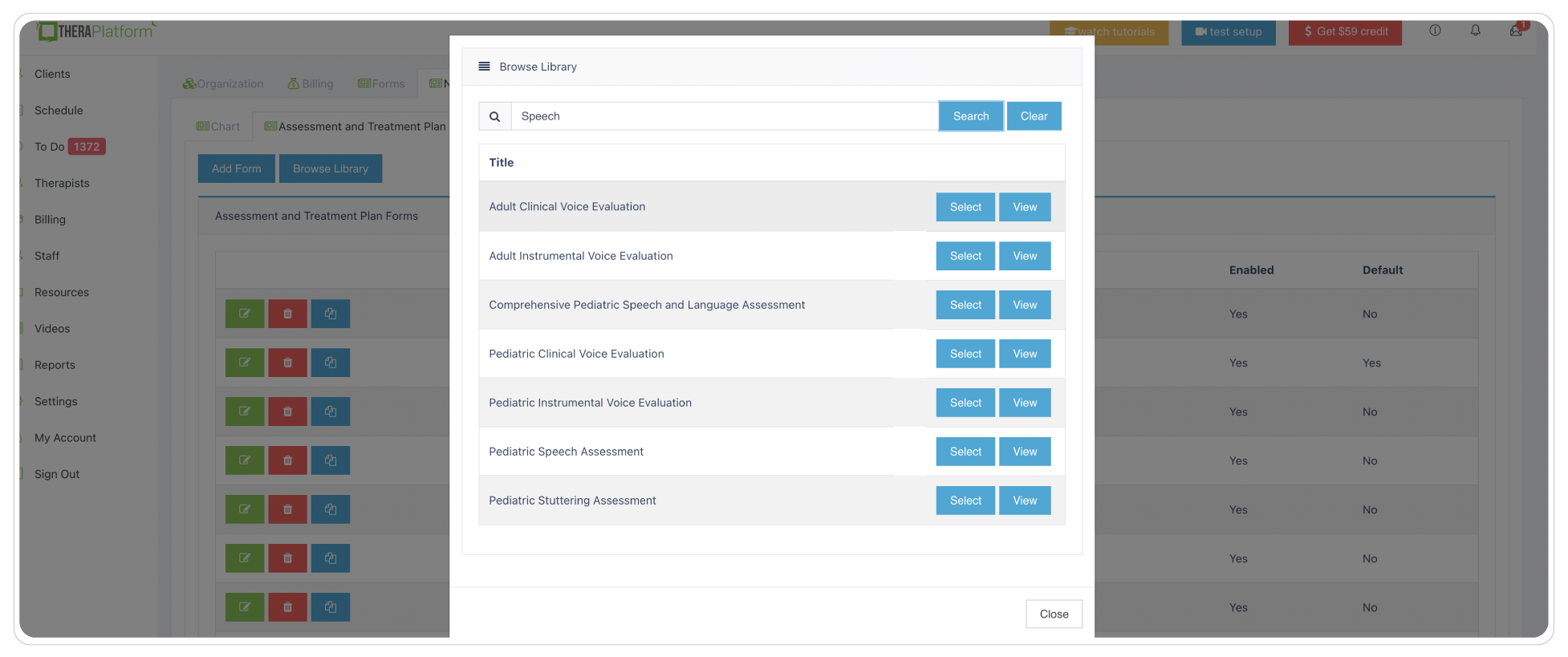
Search TheraPlatform’s built-in note therapy note template library based on your profession and edit templates to meet your needs.
Flexible note template builder
Different SLPs have their own ways of documenting speech therapy sessions. Some love SOAP note templates to help organize subjective, objective, assessment and plan information. Other SLPs prefer just one field that allows them to type their narrative. While other SLPs incorporate checkboxes on their note templates for repetitive information such as techniques used or mental status. Having a robust and easy-to-use note template builder is the key to having such flexibility.
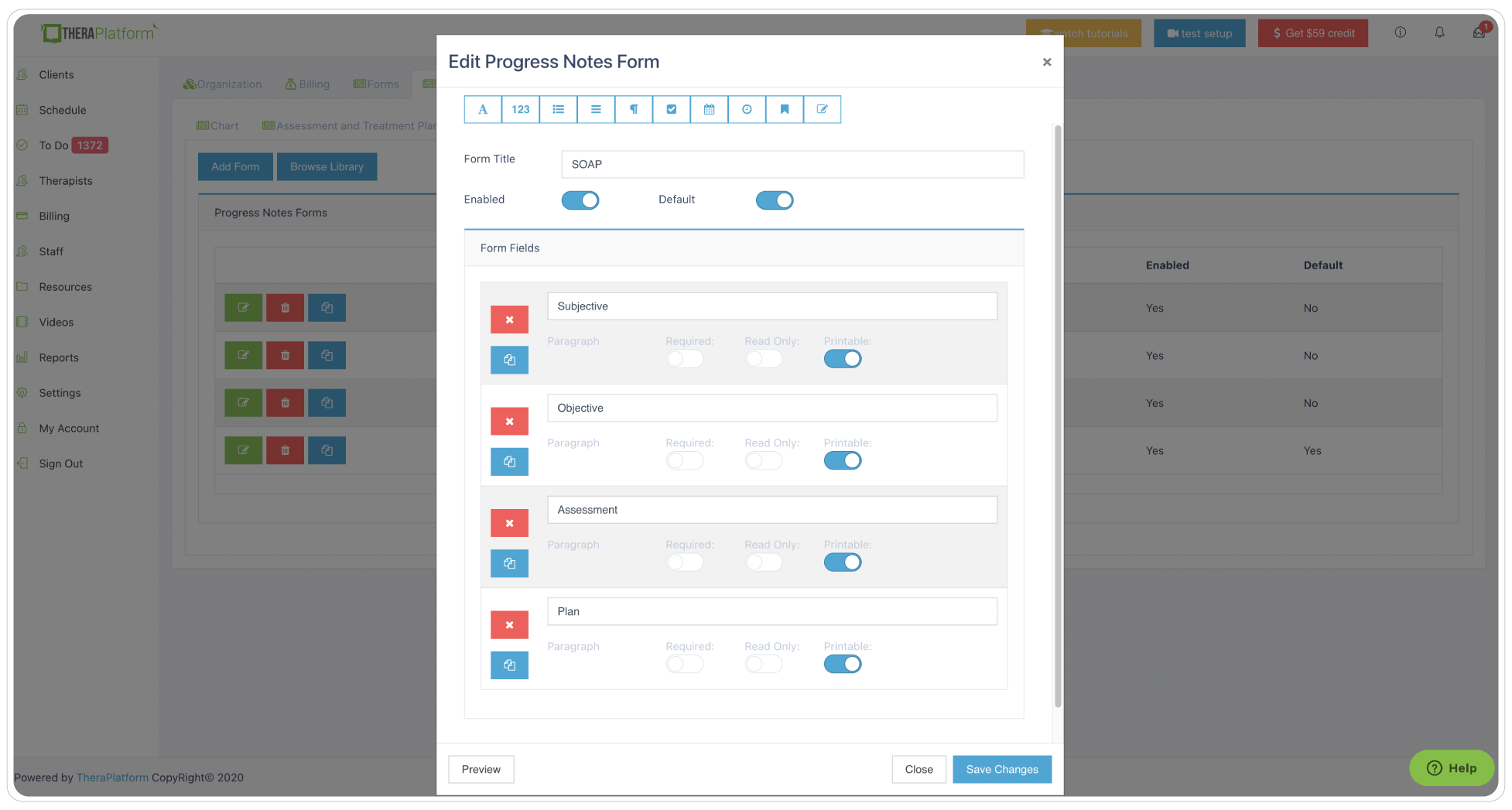
Leverage existing templates or make them your own with new fields like checkboxes, buttons or pick lists.
HIPAA-compliant and secure storage of speech therapy notes
Whether you are a covered entity or not under HIPAA, creating and storing your speech therapy notes in a secure, encrypted system to prevent breaches will ensure your client’s data is safe and give you peace of mind. TheraPlatform follows bank-level security standards and provides private practices with a signed BAA.
Start 30-day Free Trial and explore TheraPlatform. HIPAA Compliant Video and Practice Management Software for Therapists.
Easily and securely share your speech therapy notes with clients
You may have clients on your caseload who request speech therapy notes for their own records, or superbill clients who need them in case of insurance audit. Having a secure way to share your notes is no brainer.
TheraPlatform’s EMR for speech therapists, allows SLPs to share speech therapy notes with clients via client portal in a HIPAA-compliant and secure way.
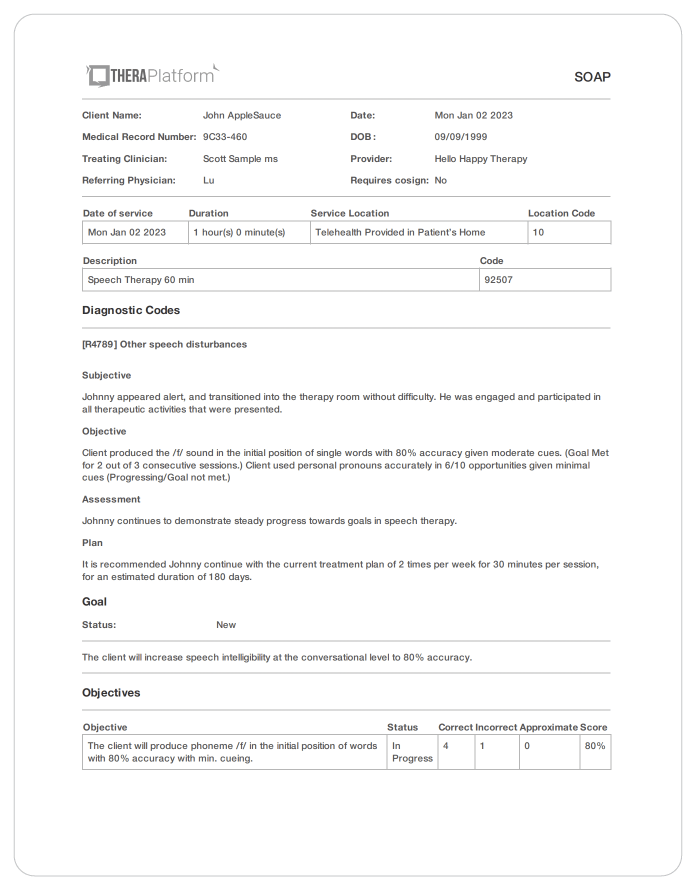
Speech therapy SOAP note created with TheraPlatform. Therapists can share notes with clients with a couple of clicks of a button.
Electronically request signatures from your clients on your speech therapy notes.
TheraPlatform's Pro and Pro Plus plans offer documentation features with the ability to request signatures from clients on notes. Your client can also download and print this document.
Copy notes from previous sessions
Some information that SLPs type on SOAP notes might repeat from session to session and a copy note feature on TheraPlatform, allows clinicians to copy notes from previous sessions. They can still edit the copied note and add more information to it too.
Fax your notes from your clients’ chart with a click of a button
Having efax integrated into an EMR such as TheraPlatfrom eliminates maneuvering between two services, saves time and lowers cost as incoming and outgoing documents like SOAP notes, and other documents are sent via efax.
Remember, clear, consistent, and concise are words speech therapists should keep in mind when writing an SLP SOAP note. SOAP note templates like those offered on TheraPlatform can make writing SLP SOAP notes much easier. In addition, TheraPlatform has a number of features to make practice management more efficient including scheduling, billing and claims. TheraPlatform, an all-in-one EHR, practice management and teletherapy tool was built for therapists to help them save time on admin tasks. They also offer a 30-day free trial. No credit card required.
Resources
More resources
- Therapy resources and worksheets
- Therapy private practice courses
- Ultimate teletherapy ebook
- The Ultimate Insurance Billing Guide for Therapists
- The Ultimate Guide to Starting a Private Therapy Practice
Free video classes
- Free mini video lessons to enhance your private practice
- 9 Admin tasks to automate in your private practice


