DAP notes

DAP notes are one type of clinical note that counselors need to write and review and professionals in almost every therapeutic field have to keep progress notes. Many just wing it and put down whatever they want. But it can be helpful to format and organize your notes to ensure that you don’t leave anything out. DAP notes provide mental health professionals with a guide for arranging pertinent information from psychotherapy sessions. Here is a DAP note primer.
What is a DAP note?
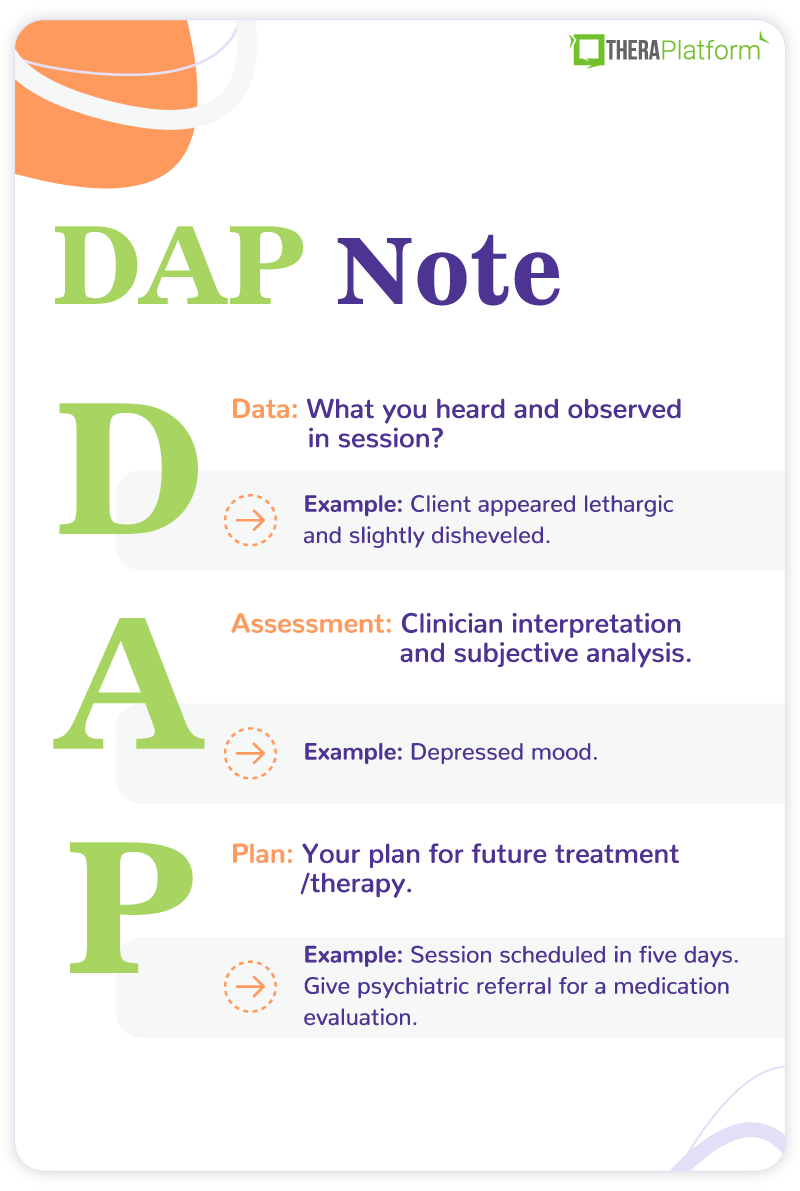
DAP is an acronym for Data, Assessment, and Plan. It is a simple and comprehensive template to help organize your notes. It is important to recognize that a DAP note is a progress note, not a personal psychotherapy note. That means it is part of the official record and can be shared with others. Let’s explore each part of the DAP note.
Data
The data component of DAP notes includes everything you heard and observed in the session. It is a review of all the information gathered. You want this section to be as objective and factual as possible. Most of this information is client self-report but clinician observations also provide valuable information. For example, they may note that a client “appears agitated”. Additionally, the data section includes interventions that the professional used in the session and the client’s response. This is similar to what you would find in a BIRP (Behavior, Intervention, Response, and Plan) note but the DAP note does not have separate sections. This is also where you would include client quotes that provide important information.
Here are some questions that are frequently answered in the data section of a DAP note:
- Why is the client here?
- How do they present themselves, including their mental status?
- Are they reporting or experiencing symptoms?
- What important events have occurred recently (since last session)?
- How have they responded to interventions from previous sessions?
- What is their behavior toward treatment? For example, are they doing their homework or missing sessions?
An overall question that summarizes this section is “what did I see and hear?”
Assessment
The assessment portion of the DAP note reflects clinician interpretation. This is when you get to flex your clinical muscles and figure out what is going on with your client. Unlike the data section, it is primarily based upon subjective analysis.
Here are some important questions to answer in the assessment section:
- Do you feel the client is making an effort to address their issues?
- How does the data reflect attention to their treatment goals?
- Are they making progress?
- How do they respond to interventions in session?
- Are there concerns about self-harm or harm to others?
- Does the data indicate a particular diagnosis or issue to be addressed?
- Is there any formal assessment information from testing or a screening measure?
In other words, “what does the data mean?” The assessment section is a natural follow-up to the data. Whoever is reading your note should be able to see the reasons for your assessment based on the data.
Start 30-day Free Trial and explore TheraPlatform. HIPAA Compliant Video and Practice Management Software for Therapists.
Plan
The final portion of the DAP note is the plan for future treatment. It may involve what you want the client to do next as well as what you, the therapist, want to accomplish. For instance, you may write that the client is to complete a homework assignment or that you need to contact their psychiatrist about their medication. Keep in mind, this segment is not the entire treatment plan. It is simply the goal from one session to the next. However, it may include changes or new directions to the overall treatment plan.
Some possible questions answered in this section include:
- When is the next appointment?
- Is there any homework assigned to the client?
- Any consultation needed with other professionals (e.g., a psychiatrist)?
- Any planned future interventions?
- Any changes in client goals or treatment plan?
The plan section answers the overall question, what will you do next?

What is the difference between DAP notes and SOAP notes?
If you have ever taken progress notes as an employee of a large organization, you may have been asked to use the SOAP format. The SOAP (Subjective, Objective, Assessment, and Plan) note is probably the most popular format of progress note and is used in almost all medical settings.
Tips for Taking DAP Notes
Make It a DARP Note?
Don’t Write Too Much (or Too Little)
Write Your Notes Immediately After Session
Modify Your DAP Note
Follow the Treatment Plan
Know Your Audience
Ask yourself, who is likely to read this note? Because this is not a personal psychotherapy note, it needs to be professional in tone. At the same time, your language should be easily understood by anyone who reads the note, regardless of their education level. While you may sometimes feel like writing progress notes is inconsequential, the information in the note may be used for important purposes. The DAP note, for example, could be used to decide a client’s medication regimen or as part of a malpractice civil suit. That means you don’t use slang terms unless you are quoting a client. As any lawyer will tell you, once it is written down, it is part of the permanent record. Proceed accordingly.
Therapy notes can be tedious, but there are ways to simplify them including centralized locations, workflow and templates.
Watch the video below on how to save time on therapy notes
Start your free trial now
Review Your Notes
This sounds like common sense, but it is easy to rush through note writing and never give it a second glance.
- First, notes should be proofread for spelling and grammar. One of the strengths of writing notes online is that spelling and grammar can be easily reviewed.
- Second, is the tone professional and objective?
- Next, notes should be checked for content. Did you say everything you wanted to say or leave out anything important? Also, is what you are trying to say easily understood?
- Finally, ask yourself, would you be okay with this note if another professional saw it? How about the client?
Although you may not have time to inspect your notes right after you write them, reviewing them at the end of the day is good practice.
DAP notes examples
The following DAP note example involves someone with depressive symptoms:
Name: Jane Doe Age: 25 Date: 9/15/2022
Data: | Client appeared lethargic and slightly disheveled. Hair did not seem to be brushed and clothes were wrinkled. She reported that she had been cutting her thighs with a razor blade but denied suicidal intent or plan. She said the cutting makes her feel better. The client reported that she has been feeling a lot of financial and work stress. She would like to leave her job but feels she can’t due to the loss of income. Additionally, she is having trouble with a romantic relationship. She said that she is experiencing conflict with her mother and sister and can’t turn to them for advice. |
Assessment: | Depressed mood. She is under a lot of situational stress with limited emotional support. She also has a history of depression in her family. Denies suicidal ideation and has no history of suicidal behavior but is self-harming as a coping measure. When this therapist brought up the possibility of taking anti-depressant medication, she said she would consider it. |
Plan: | Session scheduled in five days. Give psychiatric referral for a medication evaluation. Continued assessment of self-harm and potential suicidality. Advise DBT skills to aid coping. |
The second example of a DAP note is for a client experiencing anxiety symptoms:
Name: Jane Doe Age: 40 Date: 9/25/2022
Data: | Client appeared a bit agitated. He was fidgeting and bouncing his leg. He reported difficulty sleeping because of an inability to turn off the worries in his head. He said he avoided a work happy hour because he was afraid of being judged. He also is having trouble with some of his mother’s political and cultural views but does not say anything because he doesn’t want to cause problems. He did not complete the thought record homework given last session. |
Assessment: | Client has significant anxiety in several areas of his life. His avoidance of conflict and social situations is only increasing his worries. Client does not seem highly engaged in therapy. Would rather stay in his anxious space than risk the consequences of change. Appears a bit unmotivated and stuck in his progress. |
Plan: | Session scheduled for next week. Reassigned thought record homework. Assigned daily practice of relaxation exercises. No further work will be given until the client shows more consistency with present obligations. |
Improving DAP notes with EHR software
EHR software and practice management tools, such as TheraPlatform, offer numerous advantages in creating accurate, efficient, and organized DAP (Data, Assessment, and Plan) notes.
Top 7 benefits of using EHR for DAP notes
Manually writing and storing DAP notes can be cumbersome for many therapists. That process can be further exacerbated by simple document requests that include locating, faxing or scanning documents. Automation features like customizable templates, secure storage, easy sharing, duplication, electronic signatures, and efax integration, streamline the DAP note process, optimizing therapy documentation and workflows.
1. Consistent notes with template library: EHRs equipped with a library of note templates enable therapists to create standardized and concise DAP notes quickly. This feature ensures consistency across notes, making it easier to review client progress. Additionally, EHRs provide centralized storage and management of notes, enhancing accessibility and organization.
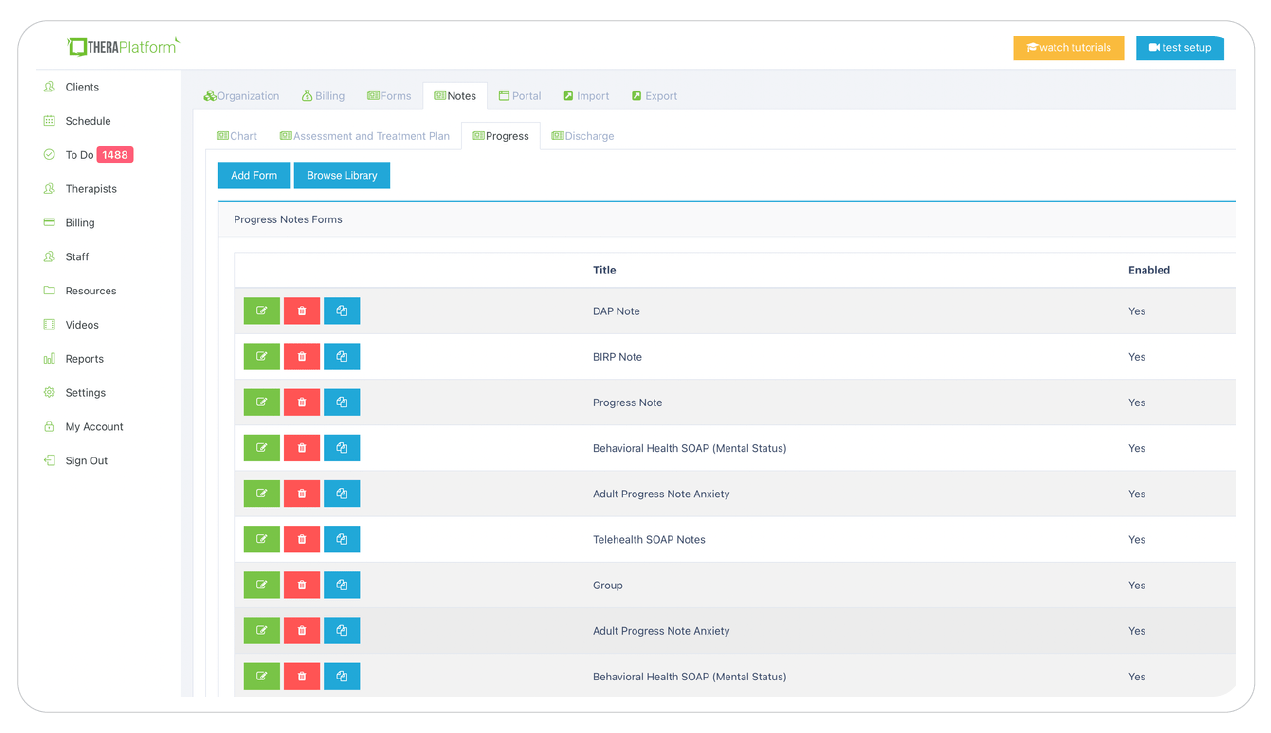
Screenshot of TheraPlatform’s built-in therapy note template library. DAP notes are one of dozens of types of templates that can be used as is or modified to meet the needs of a therapist in private practice.
2. Customizable notes: Not all EHRs offer customizable note templates tailored to therapists' unique needs. However, with a robust and user-friendly note template builder, therapists can customize DAP note templates to align with their preferred note-taking style. This flexibility allows for efficient data entry, whether therapists prefer separating Data, Assessment, and Plan sections or using a single note field or checkboxes for mental status or techniques.
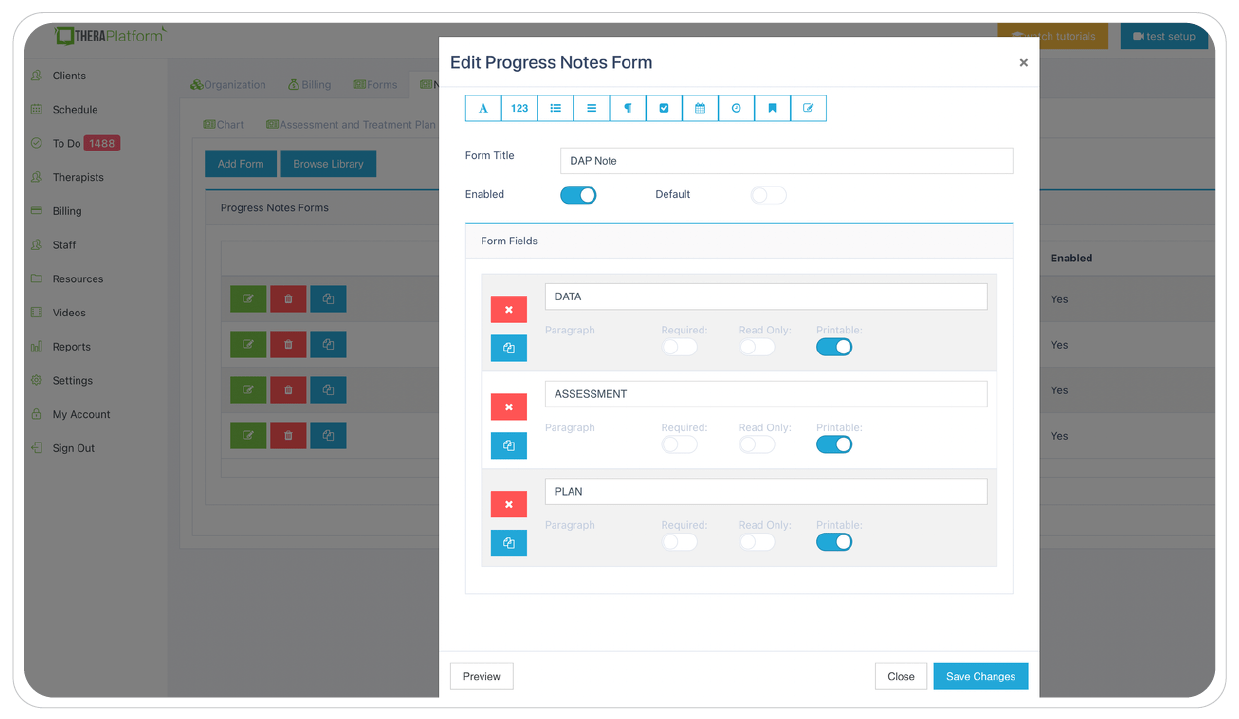
Screenshot of TheraPlatform’s DAP notes form builder. Easily complete DAP notes based on templates and update for the specific needs of the session.
3. HIPAA-compliant DAP note storage: EHRs prioritize data security by implementing bank-level encryption to safeguard DAP notes and other client information. TheraPlatform, for instance, ensures HIPAA compliance by offering signed, legally-binding Business Associate Agreements to protect Protected Health Information (PHI) between compliant entities.
4. Seamless DAP note sharing with clients: Clients may request access to their DAP notes to better understand their treatment or keep them for record-keeping purposes. Using an EHR, therapists can securely share DAP notes with clients, saving time compared to paper-based practices. TheraPlatform, a HIPAA-compliant EHR for therapists, facilitates secure DAP note sharing with clients.
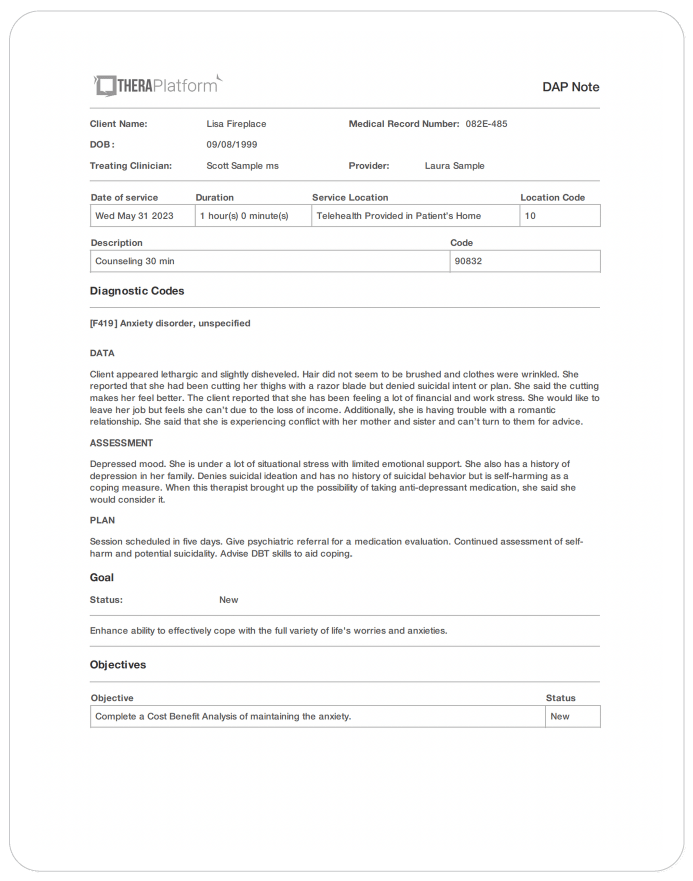
Screenshot of the popular DAP note template created with TheraPlatform. Built-in templates allow for consistent and standardized note-taking.
5. Duplicate DAP notes: In cases where the data remains the same across multiple sessions, duplicating DAP notes can save time. This feature is particularly useful when clients exhibit repetitive behaviors or show minimal progress, allowing therapists to refer back to previous notes for accurate documentation.
6. Client signatures made easy: EHRs streamline the process of requesting client signatures. TheraPlatform's Pro and Pro Plus plans enable therapists to request electronic signatures directly on DAP notes. Clients can conveniently download and print the documents requiring their signatures.
7. Easier faxing: TheraPlatform offers efax integration as an add-on feature, eliminating the need for toggling between multiple services. This integrated solution allows therapists to send and receive documents, including DAP notes, via fax directly from TheraPlatform. Additionally, received faxes can be easily filed under the respective client's charts.
By leveraging the capabilities of EHR software like TheraPlatform, therapists can enhance the accuracy, efficiency, and accessibility of their DAP notes, allowing them more time to enhance client care.
Theraplatform supplies clinicians with all the necessary HIPAA-compliant practice management resources to make documentation and billing a little less painful. TheraPlatform, an all-in-one EHR, practice management and teletherapy tool was built for therapists to help them save time on admin tasks. Sign up for a free 30-day trial today.
More resources
- Psychotherapy notes
- SOAP notes for counseling
- Crunched for time? Try concurrent documenting
- Therapy resources and worksheets
- Therapy private practice courses
- Ultimate teletherapy ebook
- The Ultimate Insurance Billing Guide for Therapists
- The Ultimate Guide to Starting a Private Therapy Practice